
by Dr. John Carosso, Psy.D.

Article at a Glance
- Early diagnosis and consistent treatment dramatically change outcomes. Undiagnosed ADHD compounds academic struggle, peer rejection, and self-esteem damage, which becomes progressively harder to reverse over time.
- Two-thirds of children with ADHD develop into adults with no significant mental health disorder. An ADHD diagnosis does not predetermine your child's future.
- Parental support and advocacy are more powerful predictors of success than ADHD severity itself. What parents do after diagnosis matters far more than the diagnosis itself.
- Adolescence (13–18) is the hardest and most critical window for intervention. This is when ADHD peaks in impact, but it's also when intervention creates the most lasting change.
- Untreated ADHD creates a cascade of secondary damage across all life domains. Children without treatment are 11 times more likely to drop out of high school and face ongoing employment and mental health struggles.
- Girls with ADHD are diagnosed 5–10 years later than boys, resulting in years of accumulated self-doubt and academic damage. Don't wait for teachers to notice; get your daughter evaluated if you suspect ADHD.
- Comorbid anxiety and depression dramatically worsen outcomes and require separate treatment. Treating only the ADHD while ignoring emerging anxiety or depression won't work.
- Educational accommodations (IEP or 504 plans) predict significantly better academic outcomes. Parents who advocate for formal written accommodations provide their children a measurable advantage.
- One stable, affirming relationship with a caring adult is the single strongest protective factor for resilience. This relationship matters more than medication, the perfect school, or any other intervention.
- Multimodal treatment (medication + therapy + coaching) produces noticeably better outcomes than any single intervention alone. Consistency across all three domains is what creates real change.
When I meet with parents to discuss an ADHD diagnosis, I’m frequently asked the following two questions: “Will my child outgrow this?” And, “How will this affect their future?” These are very real and legitimate questions. My response to these two questions is more hopeful and more honest than some sources will admit.
In my judgment, I assess the long-term prognosis for children with ADHD as cautiously optimistic.
Research shows that 60–65% of children continue to manage ADHD symptoms into adulthood, though for many, those symptoms become less visible. Even better: about two-thirds of children with ADHD go on to lead successful adult lives with steady jobs, healthy relationships, and meaningful education. But here's the realistic part: without early diagnosis and consistent treatment, the path gets a lot harder. Untreated ADHD increases the risk of dropping out of high school (32% vs. 15% in the general population), struggling with employment, and battling mental health challenges like anxiety and depression.
So, what determines which path your child takes? That's precisely what we'll explore together in this article: How to maximize your son or daughter's long-term prognosis.
We're going to walk through what the research actually says about ADHD outcomes, the factors that predict brighter futures, the challenges that can derail progress, and most importantly, what you as the parent can do to help shape your child's long-term trajectory.
The Science Behind ADHD Persistence: Why It Doesn't Just Disappear
Let's start with the neurological reality. ADHD isn't something kids "catch" and then recover from like the flu. It's a neurodevelopmental difference, meaning it's baked into how their brain is wired from the start.
This matters because it explains why ADHD doesn't magically vanish when a kid turns 13 or graduates high school. The brain differences that cause inattention, hyperactivity, and impulsivity don't disappear. What does change is how those differences show up in daily life and how much they impact functioning.
Here's the research breakdown. When experts follow children diagnosed with ADHD from childhood into adulthood, they observe remarkably consistent patterns:
Into adolescence: Between 50 and 80% of children continue to show ADHD symptoms that are clinically significant, meaning they're causing real problems with school, friendships, or home life.
Into adulthood: Between 35 and 65% of those kids continue to meet diagnostic criteria for ADHD or show what's called "subsyndromal ADHD" (that's research-speak for "not quite meeting all the diagnostic boxes but still struggling").
By the mid-20s: About 29–35% continue to have full ADHD diagnoses. Another significant chunk has what we call "partial persistence," meaning they're managing some symptoms well but still dealing with executive function challenges, relationship friction, or other lingering effects.
And here's what matters: two-thirds of children with ADHD show no evidence of mental disorder by their mid-20s. That's the headline the research gives us. Most kids do okay. Many do really well.
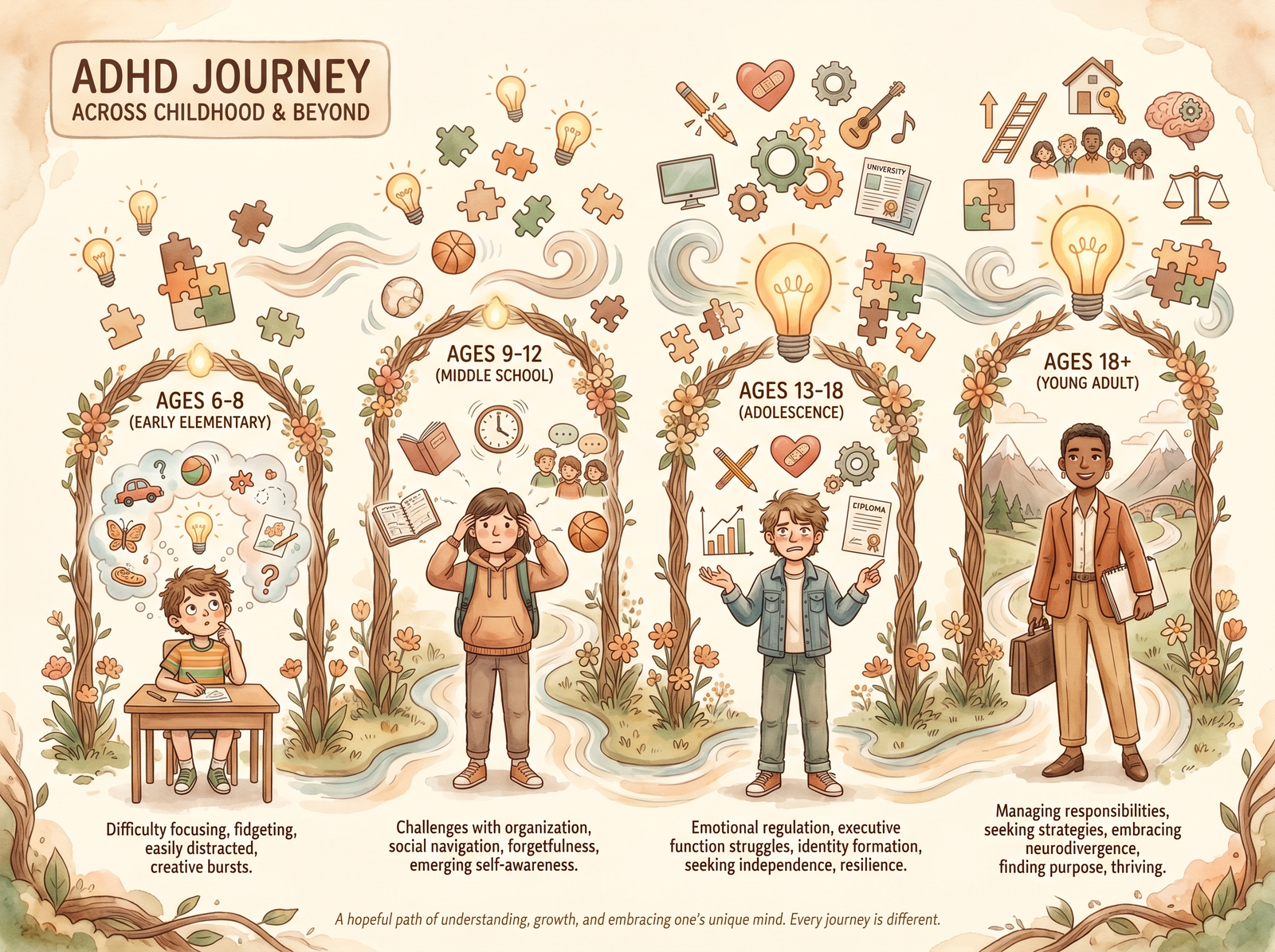
ADHD doesn't disappear—it transforms across childhood. Here's what to expect at each stage.

What the Research Actually Shows: Outcomes Across Life Domains
Alright, let's get into the real-world data. How do children with ADHD actually fare as they grow up?
Educational Outcomes
This is where I need to be straight with you. Children diagnosed with ADHD drop out of high school at a much higher rate, about 32%, compared to 15% in teens with no psychiatric disorder. That's significant.
College enrollment? Roughly 50% of young adults with ADHD attend vocational or junior college, compared to 18% of non-ADHD peers. And four-year college? Just 15% of young adults with ADHD hold a bachelor's degree versus 48% of their non-ADHD counterparts.
But, and this is important, it does not mean ADHD kids can't or won't graduate. Here's what that research also found: some children with ADHD go on to complete Master's degrees. Some go to medical school. Some become accountants, stockbrokers, entrepreneurs, and teachers. The career ceiling isn't lower. It's just that more kids with untreated ADHD hit obstacles along the way.
Occupational Outcomes
Young adults with ADHD face significant employment difficulties by their mid-20s to early 30s: they are 11 times more likely to be unemployed or out of school, 4 times more likely to hold unskilled jobs, 61% more likely to have been fired, and 33% more likely to have been laid off.
When they do work, they earn roughly $2 per hour less than non-ADHD peers. That's real money over a lifetime.
The Social & Mental Health Picture
This is where the broader perspective comes into play. Children with ADHD often struggle with social relationships. They're more likely to be excluded from peer groups at school, which affects self-esteem. This type of pain hits different than academic struggles. Self-esteem damage compounds over time. And when you combine social rejection with academic failure, you get fertile ground for anxiety and depression to take root.
Research shows adults with ADHD have significantly higher rates of depression and anxiety disorders compared to the general population. They're also at higher risk for substance abuse, not because ADHD causes addiction, but because untreated ADHD increases impulsivity and struggling kids sometimes self-medicate.
But Here's the Hopeful Part
Despite all those statistics, two-thirds show no signs of mental disorder by their mid-20s. Most are employed, even if employment patterns have been rocky. Many have positive relationships, stable housing, and a sense of direction.
The difference? The key factors are early intervention, consistent treatment, and parental support during the critical years.
ADHD in Girls: Why Prognosis Often Differs
Here's something that doesn't show up clearly in population statistics but shows up constantly in clinical practice: girls with ADHD often have different outcomes than boys, and part of that is because they're diagnosed years later.
Why Girls Get Missed
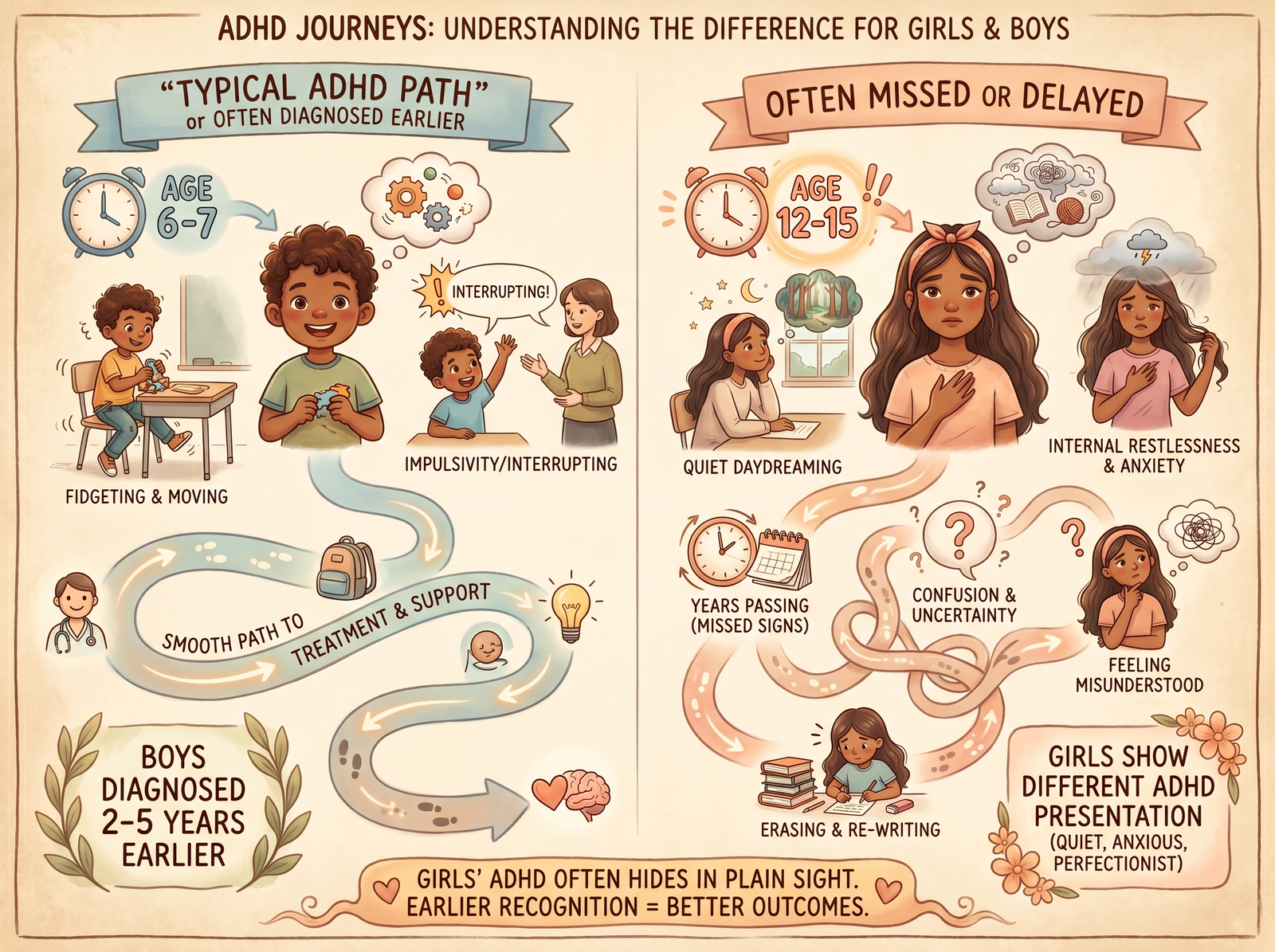
Boys with ADHD tend to have the hyperactive presentation. They're bouncing off walls, interrupting class, and getting sent to the principal's office. Teachers notice. Parents notice. Diagnosis comes at age 7 or 8.
Girls, especially those with inattentive-type ADHD, are often the quiet daydreamers or the "could do better if they'd tried" kids. They're not disrupting class. They're just sitting in the back, struggling to focus, turning in half-finished work. Some are perfectionists trying to cover up their struggles. Some are anxious about being "found out" as not being smart enough.
Result? Girls with ADHD are diagnosed on average 5–10 years after boys. By the time a girl's inattentive ADHD is caught, she's already experienced years of academic struggle, social comparison ("Why am I not as smart as my friends?"), and self-esteem erosion.
Different Outcomes, Different Challenges
Girls with ADHD tend to have higher rates of anxiety and depression than boys with ADHD. They're more prone to perfectionism, which backfires when they can't meet their standards. They're more likely to develop eating disorders or struggle with body image. Their peer relationships matter more to their sense of self-worth, so social rejection hits harder.
And here's the thing: by the time a girl gets diagnosed and starts treatment, she's got years of accumulated self-doubt to work through. Treatment addresses the ADHD, but the emotional scars take longer to heal.
What Helps
Girls with ADHD benefit enormously from having female role models and mentors who get it. They benefit from strength-based parenting, focusing on what they do well instead of constant correction. They also benefit from early intervention, which can involve expressing concerns and seeking an evaluation rather than obtaining a full diagnosis.
If you have a daughter you're worried about, don't wait. Get her evaluated. The earlier you can address it, the better her long-term outlook.
Are you skeptical about the concept of ADHD, or have questions about a diagnosis? If so, you might want to read "The Facts and Fallacies of ADHD." In it, I discuss topics such as diagnosis validity, medication safety, and discipline myths.
What Actually Changes Outcomes: The Parental Agency Layer
Okay, let's discuss the thing that separates kids who thrive from kids who struggle. It's not their ADHD severity. It's what happens after the ADHD is identified.
Early Diagnosis & Intervention Timing
Does it matter if a child is diagnosed at 6 versus 12? Research says absolutely yes. Every year of undiagnosed ADHD is a year of academic struggle, peer rejection, and self-esteem damage that compounds. A child diagnosed at 6 gets 6 years of treatment and support before high school. A child diagnosed at 12 is already behind academically and socially.
Early intervention doesn't cure ADHD, but it prevents a lot of secondary damage.
Treatment Compliance & Consistency
This is huge. Children whose parents ensure consistent treatment, whether that's medication taken every day, weekly therapy appointments kept, or coaching sessions attended, show dramatically better outcomes. It's not complicated: consistency matters.
Kids who start medication but only take it on school days, then skip it on weekends? Mixed results. Kids whose parents advocate fiercely for accommodations at school and also provide structure and support at home tend to have a much better trajectory. Much better trajectory.
Parental Coaching & Behavioral Support
You know what predicts better outcomes in young children with ADHD more than anything else? Parent behavior management training. That's research jargon for "parents learning strategies to help their child succeed."
When parents understand ADHD, they stop blaming themselves ("My child is just lazy" or "I'm failing as a parent") and instead learn how to support an ADHD brain. Reward systems that work, consequences that make sense, and communication that gets through. A structure that supports rather than hinders.
Educational Advocacy
This one's critical. Children with ADHD who have formal accommodations, an IEP (Individualized Education Program), or 504 plans show significantly better academic outcomes. This can be extra time on tests, a separate testing space, homework reminders, and behavioral check-ins throughout the day.
Parents who advocate loudly in school, who ensure their child receives these accommodations (in writing), and who follow up with teachers regularly? Well, their kids are more likely to complete high school, consider college, and believe they can succeed in life.
Family Dynamics & Emotional Climate
Here's something that doesn't always make it into research papers: the emotional tone of a home matters enormously. A child with ADHD who lives in a house filled with criticism, blame, and frustration? That kid's prognosis gets darker. They can develop shame and start believing they're broken.
A child with ADHD who lives in a house whose parents understand the condition, communicate about it openly, and offer unconditional acceptance, even while setting clear limits? That kid's resilience is strong and his outlook is entirely different.
Comorbidity Management
This is critical. Many children with ADHD also develop anxiety, depression, or sleep disorders. What about parents who treat only the ADHD while ignoring the creeping anxiety? That kid's prognosis gets harder. However, parents who consider all aspects, including ADHD treatment, therapy for anxiety, and sleep hygiene, tend to see their children thrive.
Are you interested in additional ADHD treatment strategies like time management and task completion to help bridge diagnosis → management → long-term success? My article, "ADHD: What's Executive Functioning Got To Do With It?" explores Executive Function in detail and empowers parents about what can be done to improve it.
Protective Factors: What Helps Kids with ADHD Thrive
Okay, so we've talked about what parents can do. Let's zoom out and discuss the bigger picture: what actually predicts resilience and success for kids with ADHD.
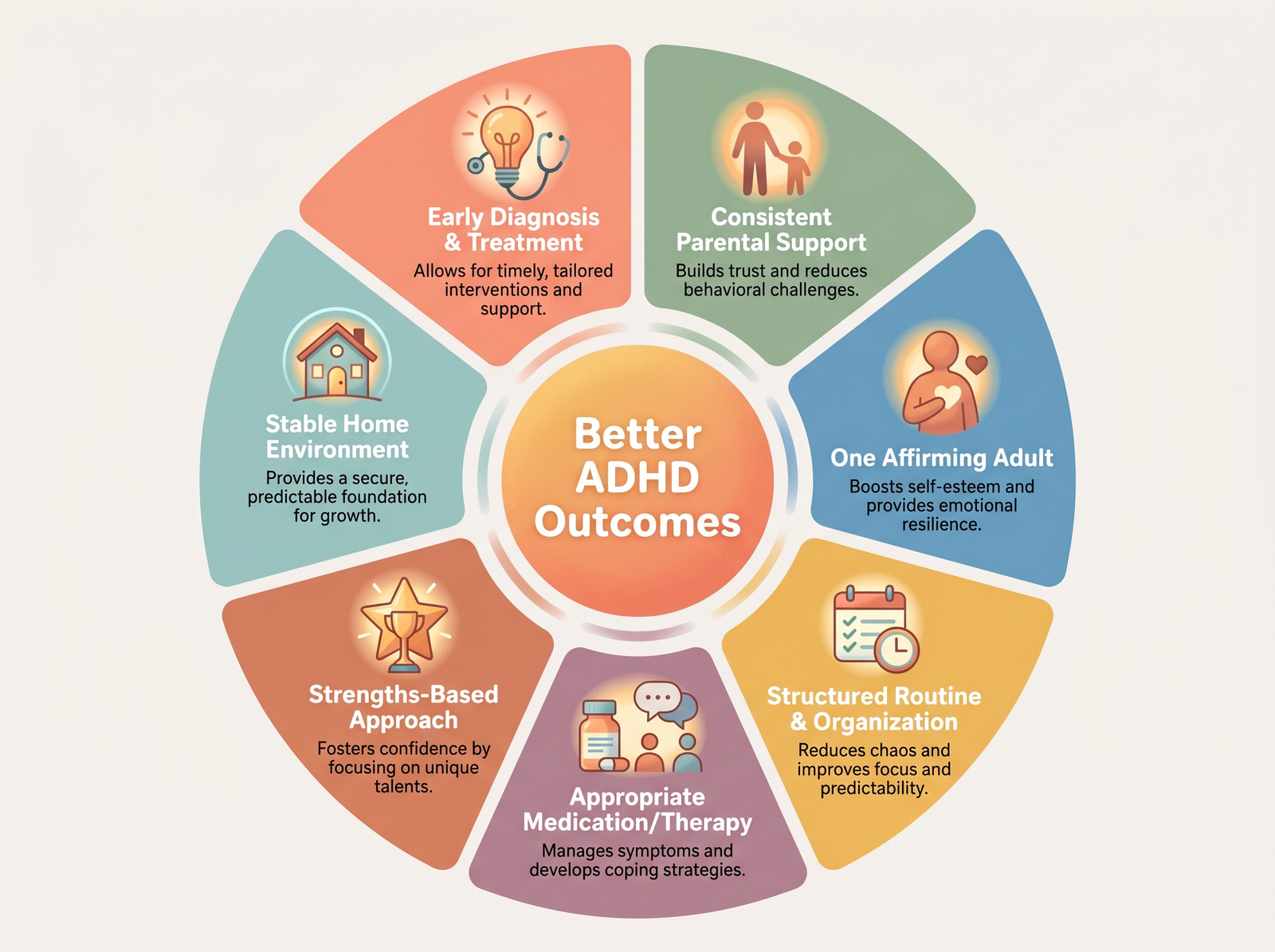
Secure Attachment to at Least One Caring Adult
This is the single strongest protective factor. Not medication. Not the perfect school. Someone who believes in the kid, sees their potential, and sticks with them on tough days.
It could be a parent, a grandparent, a coach, a teacher, or an aunt or uncle. Regardless, the research is unequivocal: children with ADHD who maintain at least one stable, affirming relationship with an adult demonstrate significantly improved outcomes across all measures.
This matters because ADHD kids get rejected a lot. Peers, teachers, and even frustrated parents sometimes reject ADHD kids. Having one person who says "You're not broken, I believe in you, and I'm not going anywhere" will change everything.
Educational Fit
Not every child succeeds in conventional classrooms. Many kids with ADHD excel in smaller classes, project-based settings, or alternative school programs.
Parents give their children a tremendous advantage when they invest energy in finding the right educational environment that allows them to thrive rather than simply choosing the most prestigious school or the one that everyone else attends.
Peer Support & Mentorship
ADHD camps. ADHD support groups. Mentorship programs. Extracurricular activities where the kid's ADHD isn't the main story. These matter because they provide kids a chance to see themselves succeeding with peers who get it or who don't judge.
A kid who spends all day in academic struggle might find community and confidence in a sports team, an art class, or a Scouts program. That confidence bleeds into other areas.
Career Alignment
Here's something intriguing: many adults with ADHD do really well in careers that match their neurology. High-energy, project-based work. Creative fields. Sales. Entrepreneurship. Emergency medicine. Things that require quick thinking and adaptability, as well as thriving under pressure.
Parents who help kids identify their strengths, not just manage their weaknesses, set them up for careers where ADHD is less of a liability and sometimes even an asset.
Consistent, Multimodal Treatment
Medication alone? Helps. Therapy alone? Helps. Coaching alone? Helps. All three together? That's where the real transformation occurs.
Kids whose families prioritize treatment consistency across domains show outcomes that are noticeably better.
What to Expect by Age: Stage-Specific Prognosis
Okay, let's talk about what prognosis actually looks like at different stages. This is because the concept of "long-term prognosis" is inherently abstract. What parents want to know is, "What should I expect this year?" And, “What's around the corner?”
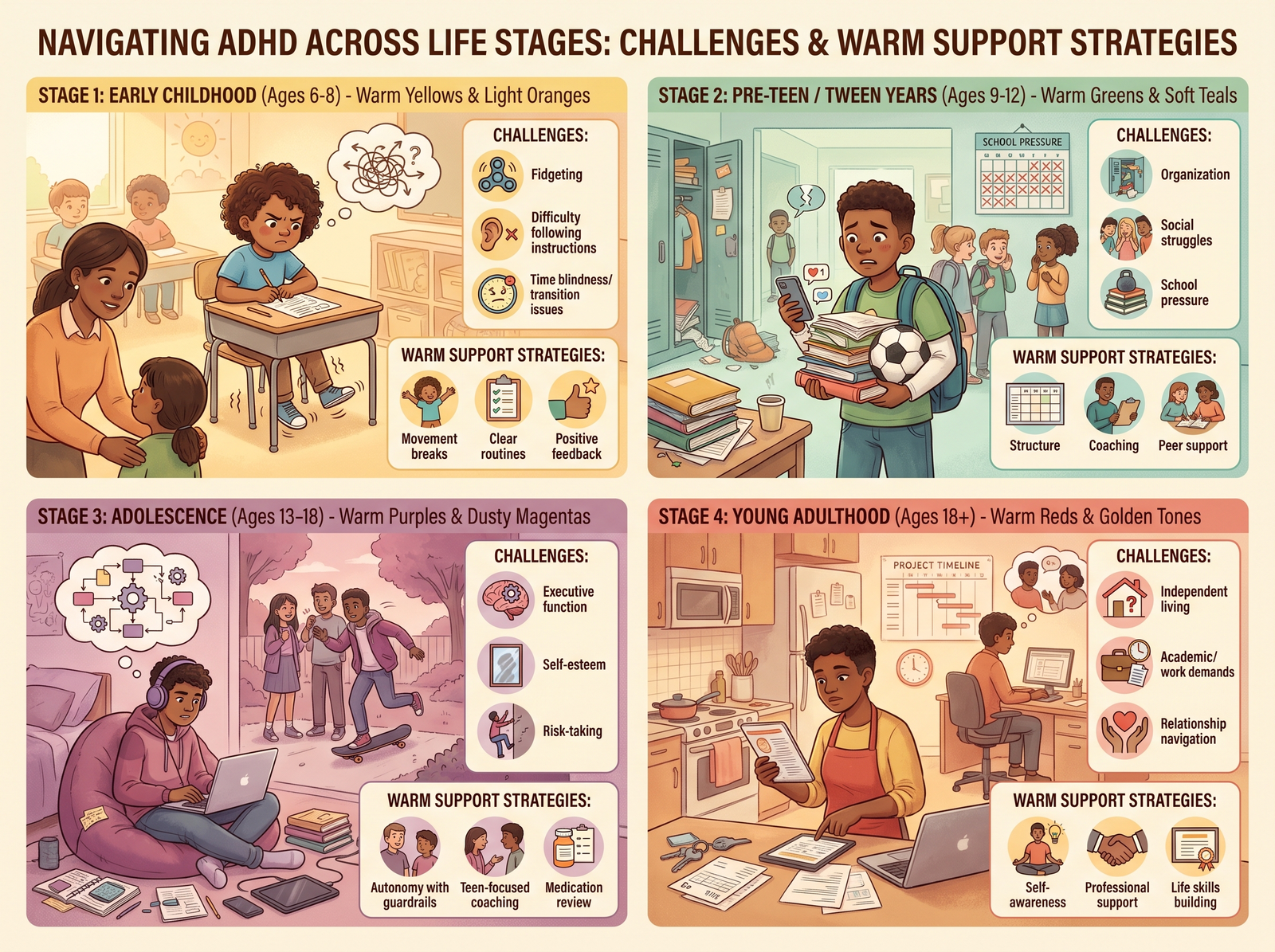
Early Childhood (6–8 Years)
This is usually the diagnosis window. “A child who got by with natural intelligence and parental scaffolding suddenly faces a classroom of 25 kids where sitting still matters.
Prognosis at this age is highly dependent on intervention speed. Early diagnosis plus immediate treatment equals better academic trajectory from this point forward. Delayed diagnosis means cumulative academic damage starting to compound.
Emotionally, kids this age are still developing their self-concept. Early intervention protects self-esteem in a way that later intervention can't fully repair.
Elementary School (9–12 Years)
This is the "trajectory-setting" phase. Academic patterns start solidifying. Is there a specific child who received early intervention and is now thriving in third grade? That momentum often carries forward. A kid who's been struggling for years by now? The gap between them and peers is getting wider.
Social dynamics matter more now. ADHD kids who are struggling academically often become targets for social rejection. That compounds the emotional toll.
The good news: treatment still helps tremendously at this age. Kids can still catch up. But it requires consistent, intensive intervention.
Adolescence (13–18 Years)
Here's the truth: adolescence is the hardest age for ADHD. This is when ADHD peaks in terms of impact and challenge.
Why? Executive function demands explode. Suddenly, a kid needs to manage multiple classes, organize their materials, plan long-term projects, regulate their sleep schedule, and navigate complex peer relationships. The brain areas responsible for all these functions (the prefrontal cortex) are still developing in ADHD brains, and in typically developing brains they're also going through rapid change.
Add puberty, which intensifies everything; identity formation, which is already complex; and peer pressure, which hits different when your brain is impulsive, and you've got a perfect storm.
Adolescence is the highest-risk period for school failure, substance experimentation, risky driving, and mental health crises. It's also the period where parental support matters most and where many parents, exhausted from years of managing ADHD, step back.
But here's the counterintuitive part: adolescence is also the window where intervention creates the most impact. Behavioral coaching, organizational skills training, mentorship, and parental support during this phase can literally change the trajectory.
Early Adulthood (18–25 Years)
Okay, here's the plot twist. For many kids with ADHD, early adulthood is when things get better.
Why? School structure is gone. Work environments are often more flexible. Adult ADHD kids sometimes discover careers and environments where their brains work. They develop their own systems. They seek out peer groups that understand and support them. They're no longer compared to a classroom standard of 25 other kids.
About 30% of individuals with ADHD actually achieve what researchers call "functional remission": they exceed diagnostic criteria or their symptoms no longer cause significant impairment.
Others don't achieve full remission but develop compensatory strategies. They learn their brain's operating manual. They build lives around their strengths.
By their late 20s and early 30s, many people with ADHD report finally feeling like they're "catching up" emotionally and finding their footing professionally. The brain regions that were so chaotic in adolescence have matured, leading to improved emotional regulation and better decision-making skills in adulthood. They've learned what works.
Risk Factors: What Worsens Outcomes
Let's be direct about what makes outcomes worse. Because understanding risk factors helps you protect against them.
Untreated ADHD
Untreated ADHD is the big one. Children without diagnosis or treatment are 11 times more likely to drop out of high school and 4 times more likely to struggle with employment. The impact compounds year by year.
Untreated ADHD doesn't stay contained to school. It affects friendships, family relationships, self-esteem, and mental health. Every year without intervention is a year of accumulated damage.
Comorbid Anxiety or Depression
When ADHD co-occurs with anxiety or depression, which happens in about 50–60% of kids with ADHD, outcomes become significantly more complicated. These kids are more likely to struggle academically and socially. They're at higher risk for suicidal ideation. Treatment becomes more complex because you can't treat just the ADHD and ignore the anxiety.
What makes a child with ADHD worse? Untreated mental health comorbidities are huge. Parental stress and criticism. Unaddressed sleep disorders. Trauma or adverse childhood experiences. Limited access to treatment due to poverty or geography.
Lack of Parental Support
A kid with ADHD whose parents don't understand the condition, blame them for their symptoms, or offer no emotional support? That kid's trajectory is noticeably worse. They develop shame about their ADHD. They internalize the message that they're broken, lazy, or bad.
Missed or Late Diagnosis
Every year a child goes undiagnosed is a year of academic and social damage. This is especially true for girls, who are diagnosed years later than boys on average.
Trauma or Adverse Experiences
ADHD plus trauma equals more complex treatment needs. Trauma can worsen ADHD symptoms and make kids more reactive and dysregulated.
Limited Access to Treatment
Poverty matters. Kids in under-resourced areas have less access to evaluation, medication, therapy, and coaching. Kids in wealthy areas have more options. That gap in access translates directly into a disparity in outcomes.
When ADHD Co-occurs with Other Conditions
Most kids with ADHD don't have "just ADHD." In addition to ADHD, they often experience anxiety, depression, sleep disorders, or learning disabilities. This issue is significant because treatment must consider the entire picture.
ADHD + Anxiety
This combination is more common in girls. The ADHD creates impulsivity and difficulty focusing. The anxiety creates perfectionism, worry, and avoidance. Together, they can create a kid who's paralyzed: too anxious to try because of fear of failure and too impulsive to stop and think before acting.
Treatment needs to address both. Sometimes anxiety medication, sometimes therapy specifically for anxiety, and always acknowledgment that treating one without the other won't work.
ADHD + Depression
This condition tends to develop over time. A child with untreated ADHD experiences years of failure, rejection, and shame. By adolescence, depression sets in. Now you've got a kid who's impulsive and unmotivated. That's a harder combination.
ADHD + Sleep Disorders
Sleep problems are super common in ADHD. And they make ADHD worse. A child who's not sleeping well is more dysregulated, more impulsive, and more emotionally reactive. Parents who address sleep alongside ADHD treatment see dramatic improvements.
Real Stories: Diverse Paths to Success
Let me give you three snapshots of what "different outcomes" actually looks like.
Sophia: Early Intervention Path
Sophia was diagnosed with inattentive ADHD in second grade. Her parents got her evaluated after her teacher mentioned she seemed to "daydream" a lot. Sophia started medication and therapy. Her school put a 504 plan in place.
By high school, Sophia was getting B's and C's, not straight A's, but showing respectable academic performance. In college, she found an environment that worked for her brain. She graduated. Now, in her late 20s, she works in marketing, a field where her ADHD-style brain is actually an asset. She has a stable job, and while she still takes medication, she's doing well.
Early diagnosis and consistent support shaped Sophia's prognosis.
Marcus: Later Diagnosis, Still Okay
Marcus wasn't diagnosed until high school. He'd been labeled a "troublemaker" for years. He dropped out at 16. By 18, he was working in a trade, and that's where his brain worked. The hands-on, project-based nature of the work suited him.
Now in his 30s, Marcus owns his own business. He's successful. His ADHD is still there, but he's built a life around his strengths, not constantly fighting his weaknesses. He wishes he'd been diagnosed earlier (could've saved himself years of shame), but he got there.
Marcus's prognosis: Later diagnosis didn't define his future because he found the right environment.
Devon: Untreated ADHD
Devon was diagnosed at age 8, but his parents didn't believe in medication. No therapy. No accommodations in school. He was smart enough that he coasted through middle school on intelligence alone.
High school hit different. By sophomore year, he was failing. By junior year, he'd dropped out. In his 20s, he struggled with employment, substance use, and relationship instability. He's doing better now after finally seeking treatment as an adult, but years of untreated ADHD took a real toll.
Devon's prognosis: Untreated ADHD created more complications than it needed to.
These aren't typical cases. Everyone's story is different. But they show that ADHD itself doesn't determine destiny. The response to ADHD does.
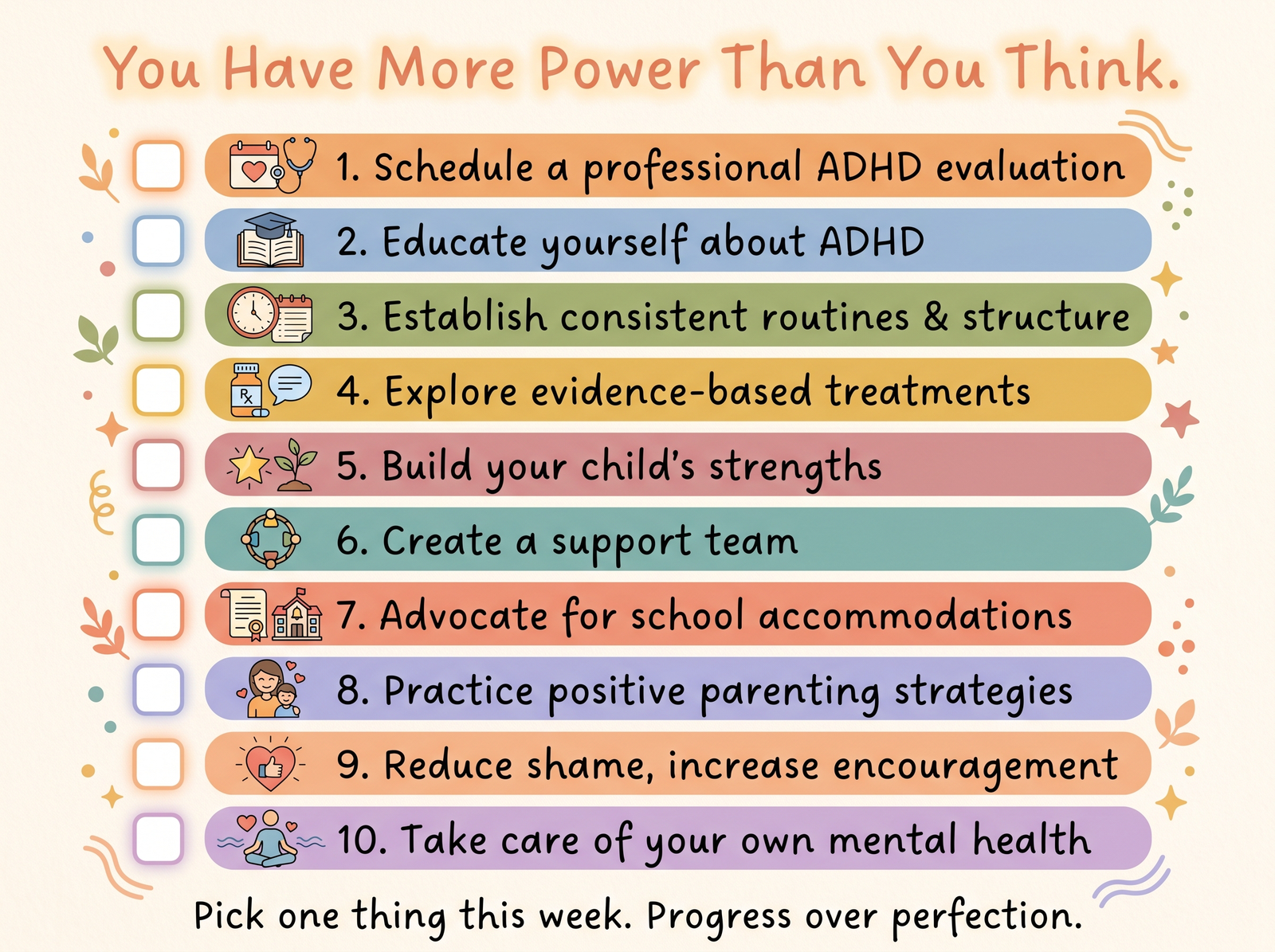
What You Can Do NOW: Your Parental Action Checklist
Okay, so you've read all the research. You understand the risk factors and protective factors. Here's what to actually do.
- Seek diagnosis early (don't wait for school to suggest it): If you suspect ADHD, get your child evaluated. Don't wait for your pediatrician to mention it. Don't wait for the teacher to mention it. An earlier diagnosis leads to faster intervention, which results in better long-term outcomes.
- Pursue multimodal treatment: Medication plus therapy plus coaching equals better outcomes than any single intervention alone. Don't choose just one and hope it's enough.
- Advocate in school (get accommodations in writing): IEPs and 504 plans matter. They predict better academic outcomes. Get your child evaluated by the school. Get official accommodations. Follow up.
- Build your own support system: You need support as much as your child does. Parent coaching. Therapist. Support groups. The extended family gets it. Don't try to manage this alone.
- Address your child's emotional landscape: Protect self-esteem. Watch for anxiety and depression. Get them addressed early if they emerge. Your child's feelings about having ADHD matter as much as the ADHD symptoms themselves.
- Treat comorbidities: If anxiety, depression, sleep issues, or learning disabilities are present, they need treatment too. Don't ignore them.
- Create predictable structure: Routines reduce anxiety and increase regulation. Your child's brain needs the scaffolding that ADHD brains don't naturally create for themselves.
- Model self-compassion: Your child learns how to think about their ADHD partly from how you think about it. If you talk about it as a flaw or a tragedy, that's what they'll believe. They will believe you if you describe it as a difference that requires management.
- Look ahead to developmental transitions: School changes, puberty, and other transitions are extra challenging for ADHD kids. Prepare and provide extra support during these windows.
- Connect with the community: ADHD support groups, camps, and mentorship programs. Places where your child sees other kids with ADHD doing okay. That normalization matters.
Below is a checklist of 10 practical steps you can use to help support your child with ADHD—from seeking a professional evaluation to practicing self-care. Download, print, and place somewhere visible as a daily reminder.
The Bottom Line: Hope + Realism
Here's what the research tells us. Your child's future with ADHD is not predetermined.
Two-thirds of children with ADHD grow into adults with no significant mental health disorder. Most find employment. Many build positive relationships and stable lives. Some thrive in ways that kids without ADHD don't.
But that doesn't happen by accident. It happens because of early diagnosis, consistent treatment, parental support, educational advocacy, and intentional protection of self-esteem during the critical years.
The prognosis for your child is positive if you act now. Not because your child needs to be fixed (they don't). But because early intervention, consistent support, and the right environment can literally change their trajectory.
If you find yourself stuck, overwhelmed, or in need of a professional opinion, don’t navigate your situation alone. Move from uncertainty to understanding—take the first step toward the answers and support you deserve. Schedule an appointment with our team and let's build a plan that fits your child, your family, and your life. Call our office at (724) 733-5757, or visit us online to request an appointment.
You can also reach out to me via email at DrCarosso@aol.com or visit acpitt.com to learn more about how we support families navigating ADHD.
Your child will be okay. And with the right support, they might be far better than just okay. Your kiddo's future isn't written yet. You're helping write it.
God bless you and your family.
Article FAQ
Yes, but multimodal treatment (medication + therapy + coaching) produces the best outcomes. Some children respond well to behavioral therapy, parent coaching, and school accommodations without medication. Others improve significantly with medication alone. But research consistently shows that the best outcomes happen when you combine approaches. Behavioral interventions plus therapy plus medication equals better results than any single intervention alone. The key is working with your child's doctor to figure out what combination works best for your child's specific situation. Some kids need medication to make therapy and coaching effective; others don't. There's no one-size-fits-all answer.
Legally and educationally, yes. In terms of identity, that's up to you and your child. Under the Americans with Disabilities Act (ADA), ADHD is recognized as a disability that may qualify your child for legal protections and accommodations at school (IEPs or 504 plans). This designation gives you power and protections. However, how your family talks about ADHD is separate from that legal status. Some families frame it as a disability that requires support. Others frame it as a neurodevelopmental difference or a different way of thinking. What matters is that your child gets the legal protections and accommodations they need and that you discuss their ADHD in ways that protect their self-esteem and help them understand themselves.
Symptoms appear early, but diagnosis usually comes when school structure demands begin (ages 6–8). ADHD symptoms exist from birth, but many children don't get diagnosed until they enter elementary school and suddenly face a classroom of 25 kids where sitting still matters. That's usually ages 6–8. However, some kids with milder ADHD or those who are naturally intelligent often go undiagnosed until middle school (ages 11–13), and girls especially frequently aren't diagnosed until high school or even adulthood (ages 14+). The earlier a child is diagnosed, the better their long-term outcome. Don't wait for official school failure before pursuing evaluation.
Structure, routine, physical exercise, sleep, and parental support are foundational. Nutrition helps but doesn't cure ADHD. Research supports several non-medication strategies: consistent routines reduce anxiety and increase regulation; physical exercise improves focus and emotional regulation; adequate sleep is critical (sleep problems make ADHD worse); a diet with stable blood sugar helps; and strong parental support matters enormously. Some families try supplements like omega-3 or magnesium, though evidence is mixed. What's clear is that diet doesn't cause or cure ADHD, though dietary adjustments can support overall wellness. The most powerful "natural" interventions are the ones that cost nothing: your presence, your understanding, consistent structure, and unwavering belief in your child.
Avoid blame-based language that suggests laziness, stupidity, or moral failure. Frame ADHD as a difference, not a defect. Language that damages: "You're so lazy," "Why can't you just focus?" "You're not trying hard enough," "You're stupid," "You're broken," "Other kids don't have this problem." These messages teach shame. Better alternatives: "Your brain works differently, and that's okay." "Let's figure out a system that helps your brain." "I know you're trying. Let's try a different approach." "You're not bad. Your ADHD is just challenging to manage sometimes." Your child already feels different and struggles. They don't need to feel blamed on top of that. The language you use shapes how they think about themselves and their future.
Severity is determined by how much ADHD symptoms interfere with your child's functioning, not by how hyperactive they are. A hyperactive kid who gets excellent grades and has friends might have mild ADHD. A quiet kid who can't focus, is falling behind academically, and is becoming socially isolated might have moderate or severe ADHD. Severity is about the impact on functioning across multiple areas (school, home, friendships, and self-esteem). Your child's doctor will assess these factors during diagnosis. What matters is understanding that severity can change with treatment. A child with moderate ADHD who receives consistent treatment might function like a child with mild ADHD. Conversely, a mildly affected child without treatment can have worse outcomes than a moderately affected child with treatment.
A meltdown is an overflow of dysregulation due to overload; a tantrum is a behavioral choice to get something. An ADHD meltdown happens when the child's nervous system becomes overwhelmed. They might cry, yell, seem inconsolable, or shut down completely. The trigger might seem small (a transition, a minor disappointment, too much noise), but the reaction is large. A tantrum, by contrast, usually has a clear goal: the child wants something and uses emotional outbursts to obtain it. Often, a tantrum stops when the child gets what they want. A meltdown doesn't stop when you provide the child what they thought they wanted because the issue is neurological overload, not unmet desire. During a meltdown, your child isn't trying to manipulate you; they're genuinely dysregulated. The response should be to stay calm, ensure safety, remove stressors if possible, and help them recover. Shame or punishment makes meltdowns worse.
Intelligence can mask ADHD for years, but eventually executive function demands catch up. Early diagnosis is even more critical. A gifted child with ADHD can rely on their innate intelligence to navigate through elementary and occasionally middle school. They get good grades despite terrible organizational skills, incomplete work, and chronic procrastination. But by high school or college, when the volume of work explodes and executive function becomes the limiting factor, they often hit a wall. Teachers assume they're lazy or not trying. The child is confused because they've always been "smart enough." This can lead to delayed diagnosis, shame ("If I'm smart, why can't I get organized?"), and sometimes crisis. Gifted children with ADHD actually need earlier intervention and more structured support because their intelligence masks the problem. Getting your gifted child evaluated for ADHD early, even if they're doing well academically now, can prevent a crisis later.
About These FAQs
The eight questions above represent some of the most commonly searched queries parents have about ADHD prognosis and management. Use these as conversation starters with your child's healthcare team and as reference points when navigating treatment decisions. Have questions you don't see here? Reach out to us anytime at www.acpitt.com/contact.
###

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}